


Epidermal growth factor receptor (EGFR), a receptor tyrosine kinase, is expressed in about 50% of patients with non-small cell lung cancer (NSCLC) [1] and is closely related to the occurrence and development of tumors. EGFR is the most frequently mutated driver gene in East Asian NSCLC patients, with a mutation frequency of 38.4%, among which the mutation frequency in East Asian female NSCLC patients is 51.1%[2]. But for Europeans or Americans, 19% of NSCLC patients carry EGFR mutations[3]. EGFR gene mutation is the most important predictor of the efficacy of EGFR kinase inhibitors (TKI) and is a prerequisite for clinical decision of whether a patient can be treated with EGFR-TKI. Both the National Comprehensive Cancer Network (NCCN) include EGFR mutation testing as a Class 1 recommendation ⁽⁴⁾.
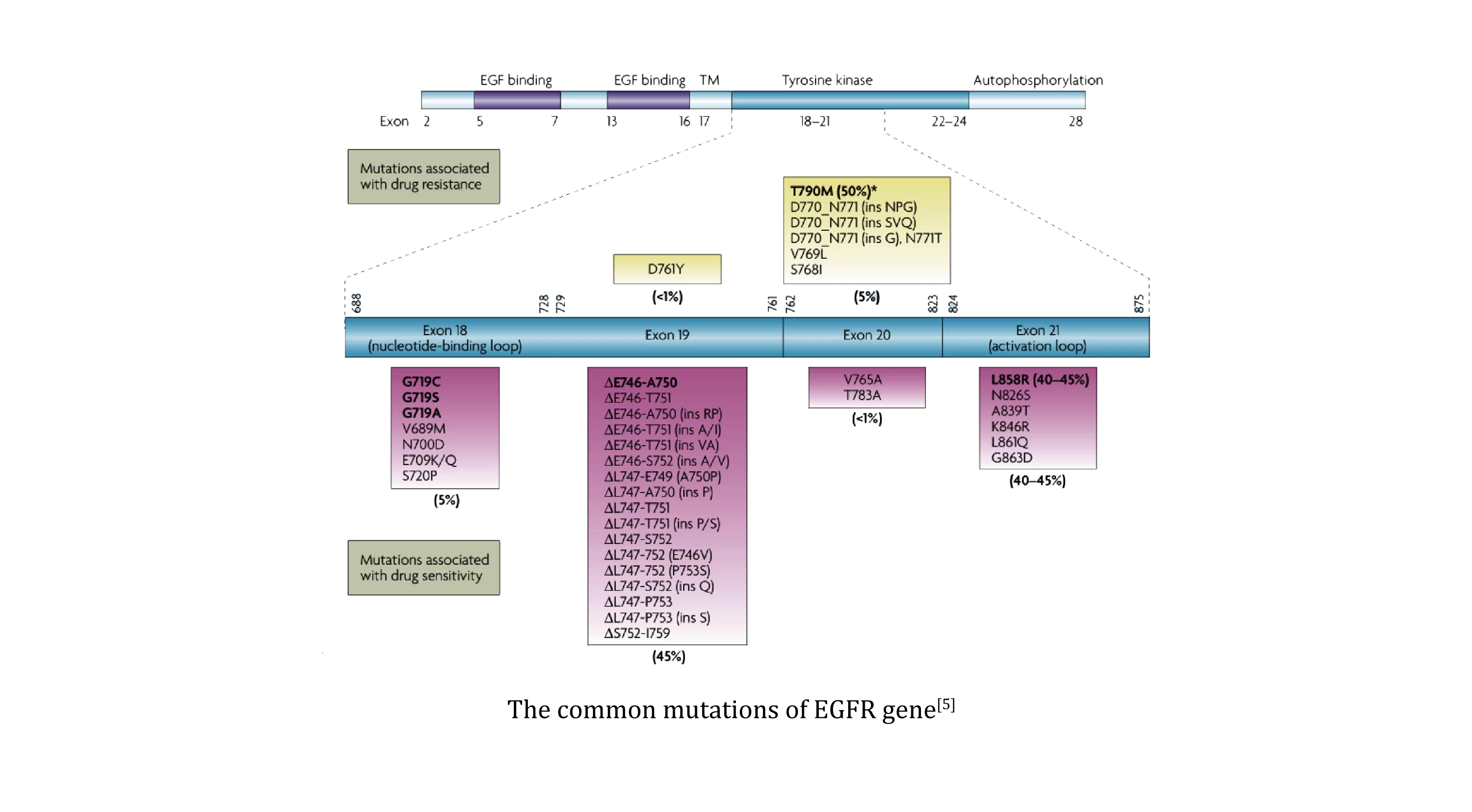
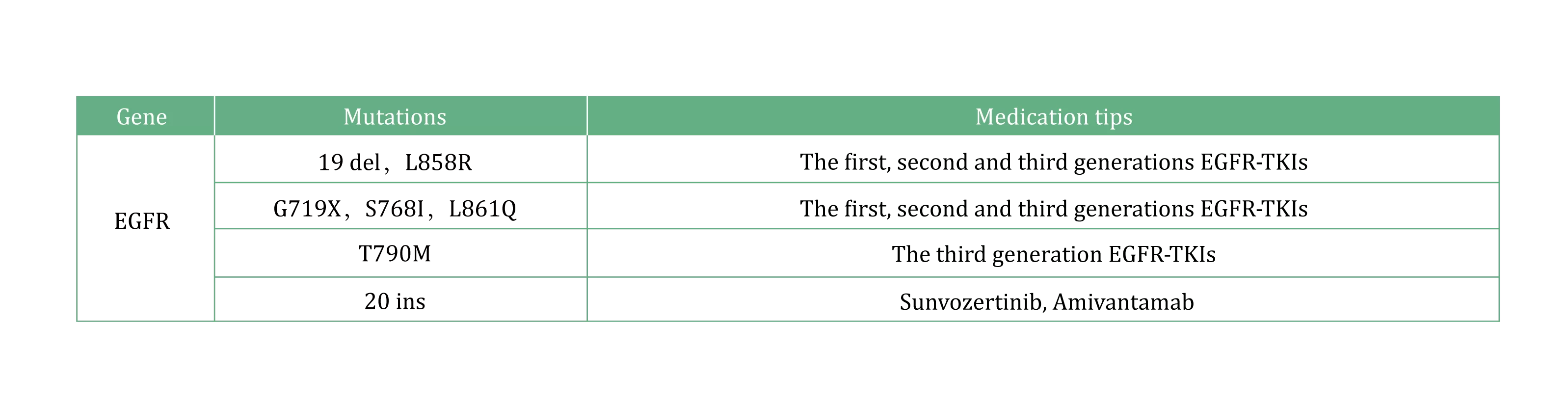
EGFR carcinogenic mutations occur mostly on exon 18-21, among which 19 del and L858R account for 85%-90% of all EGFR mutations [5], and are also the most common EGFR-TKI sensitive mutations. The T790M mutation suggests that the first and second generations of EGFR-TKI are resistant, and the third generation of EGFR-TKI needs to be used. 20 ins mutations are insensitive to conventional EGFR-TKI, suggesting the use of EGFR 20 ins inhibitors.
[1] Nat Rev Cancer. 2007 Mar;7(3):169-81.
[2] Oncotarget. 2016 Nov 29;7(48):78985-78993.
[3] World J Clin Oncol. 2021 Apr 24:12(4):217-237.
[4] NCCN NSCLC 2026 V3
[5] Nat Rev Cancer. 2007 Mar;7(3):169-81.
1.EGFR mutation detection in patients with operable stage IB-IIIA NSCLC to guide adjuvant targeted therapy.
2.EGFR gene mutation testing is performed for patients with inoperable stage III and IV NSCLC before first-line treatment, and treatment is guided by molecular classification.
3.In patients with EGFR-TKI resistance, biopsy is recommended for EGFR gene mutation detection.
High Accuracy
Closed tube testing is adopted to effectively avoid cross contamination.
High Sensitivity
EGFR gene mutations as low as 1% in 10ng DNA samples can be detected.
Comprehensive Detection
This panel comprehensively targets all druggable mutations within exons 18-21 of the EGFR gene, encompassing sensitive driver mutations (e.g., L858R, Del19), acquired resistance variants (T790M), and exon 20 insertion alterations..
1. Nucleic acid extraction
2. Set up qPCR
3. Amplification
4.Data analysis








 闽公网安备35021202000745
闽公网安备35021202000745