


Breast cancer is the leading cause of cancer incidence and mortality among women worldwide. It is a heterogeneous disease, classified into four molecular subtypes based on the presence of genetic mutations, hormone receptor status, and cellular molecular characteristics: Luminal A, Luminal B, HER2-positive, and triple-negative (Basal-like). Among these, Luminal A and Luminal B subtypes account for approximately 70% of all breast cancers, making them the most common molecular subtypes, and both are sensitive to endocrine therapy.
Endocrine therapy drugs significantly reduce the risk of recurrence and death in patients with hormone receptor-positive (HR+), human epidermal growth factor receptor 2-negative (HER2-) breast cancer. However, 20% to 30% of HR+/HER2- breast cancer patients still experience recurrence or metastasis during or after completing endocrine therapy, developing resistance to such treatment. Studies have shown that ESR1 gene mutations are the primary cause (key factor) of endocrine therapy resistance in HR+/HER2- breast cancer.
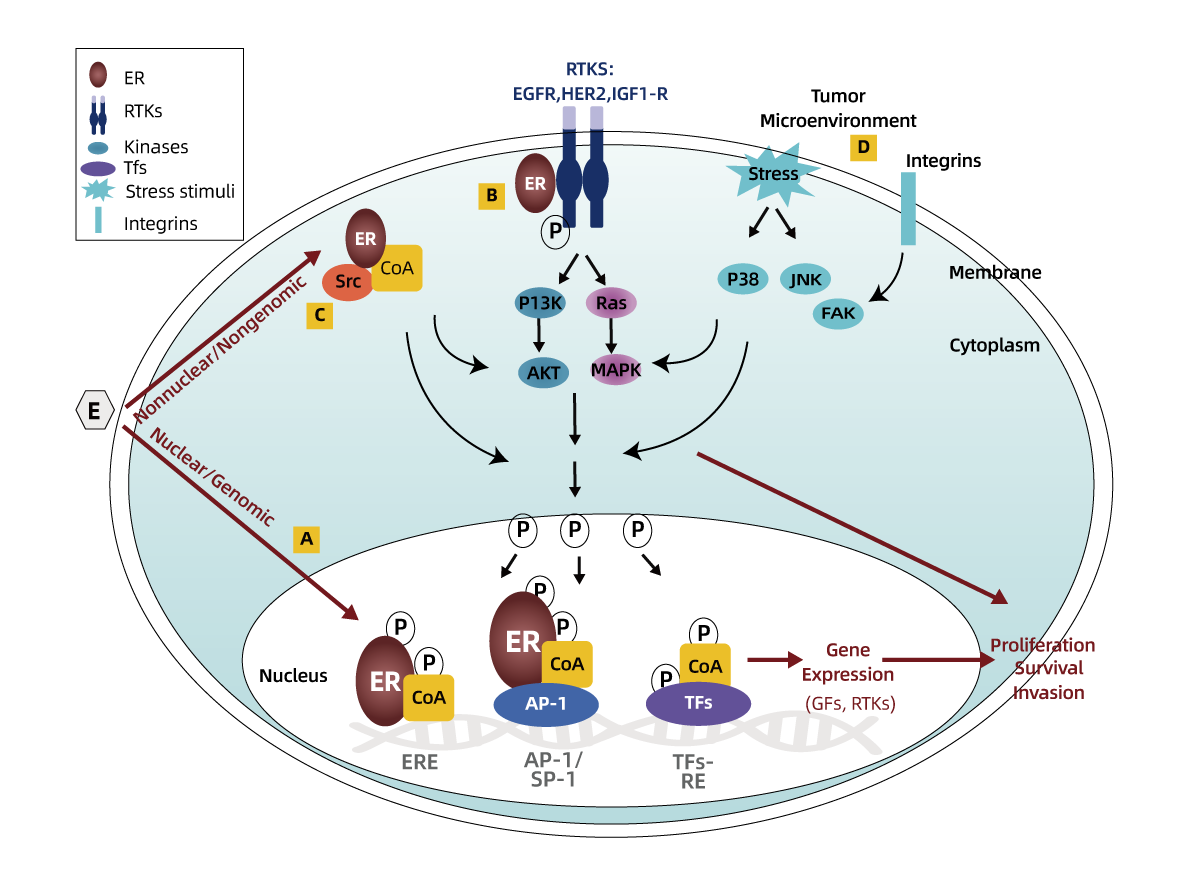
The ESR1 gene encodes the estrogen receptor (ER) protein, a ligand-dependent transcription factor. ER exerts its physiological functions through both nuclear and extranuclear pathways. In the nucleus, as a transcription factor, it directly binds to estrogen response elements (ERE, specific DNA sequences). At this point, ER typically recruits coactivator complexes (CoA), thereby regulating gene transcription. Outside the nucleus, acting like a growth factor, it binds to receptor tyrosine kinases (RTKs, such as EGFR, HER2, and IGF1-R), other signaling molecules, and coactivators (such as Src kinase). This binding can then activate multiple signaling pathways (e.g., PI3K-AKT, MAPK) and phosphorylate various transcription factors (TFs, such as AP-1 or NFκB) and coregulators, which in turn regulate gene transcription. Therefore, when the ESR1 gene is mutated, it causes abnormal ER function, leading to aberrant activation of the ER pathway. This results in abnormal cellular transcription and proliferation, as well as evasion of the inhibitory effects of endocrine therapy drugs.
The NCCN Guidelines for Breast Cancer recommend that ESR1 gene as a biomarker for HR+/HER2 breast cancer patients who have progressed following prior endocrine therapy, to guide treatment with elacestrant, imlunestrant and vepdegestrant. It is also recommended to use ctDNA as the preferred method for detecting ESR1 gene mutations.

Patients with HR+/HER2- breast cancer who are endocrine therapy-resistant, progressive, recurrent, or metastatic.
(1) Guiding treatment;
(2) Efficacy monitoring;
(3) Prognosis prediction.
Comprehensive Detection
Covers hotspot mutations, simultaneously detects 11 ESR1 gene mutation sites to guide endocrine therapy.
High Sensitivity
The kit allows the detection of 0.2%-1% of ESR1 gene mutations in 15 ng DNA samples
Liquid biopsy
Convenient sampling, more suitable for patients with recurrence, progression, and metastasis or unavailable tumor tissue
1、Nucleic Acid Extraction
2、Set up qPCR
3、Amplification
4、Data Analysis








 闽公网安备35021202000745
闽公网安备35021202000745